
Proving the Point:
Chemokines, Buckets, and Real-Time Control

For two years now, the MDNA11 story has lived somewhere between data and hypothesis. From the earliest hints of checkpoint re-sensitization to the patient anecdotes that looked like statistical outliers, the challenge has always been the same: how do you prove that a novel IL-2 is doing something no other cytokine can do?
The answer is not in a single patient case or even in a swimmer plot. It is in a coherent story where mechanism, monitoring, and survival converge. The latest evidence — from Medicenna’s AACR 2025 data, the August corporate update, the September H.C. Wainwright presentation, and a wave of translational research captured through Consensus queries — now lets us sharpen the frame.
Bridging Old and New Frames
In earlier PRISM-11 work — most visibly in Rechallenge vs. Reprogramming — we laid out four broad doors: Rechallenge, Combo Benefit, Reprogramming, and Triplet Salvage. That quadrant map emphasized long-term strategic positioning: which tumors could re-enter the checkpoint universe, which would need doublet or triplet layering, and how MDNA11 might open regulatory pathways across those landscapes.
What the latest monitoring research provides is a new level of granularity. By pairing Week-2 chemokine lifts with Week-4 cfDNA clearance, we can now tell how a response is unfolding long before the first scan. That creates three mechanistic “buckets” within the larger map: Bypass (NK-driven in deserts), Re-sensitization (CD8 renewal in CPI-refractory subsets), and Amplified Re-sensitization (MSI-H, TMB-H, viral tumors where renewal operates on an antigen-rich substrate).
These two frameworks are not in conflict — they are layered. The quadrant map still defines the strategic doors and long-term trajectories. The bucket model simply tells you, in real time, which path a given patient is taking by Week 2–4 and therefore how to operationalize trial control. The quadrant chart is the destination map, while the three-bucket frame is the dashboard telemetry.
Bypass and Re-sensitization: The Core
The most compelling way to understand MDNA11 remains the two-path model we’ve returned to repeatedly in PRISM-11:
· Bypass mode: In MHC-I–deficient tumors (immune deserts), MDNA11 activates NK cells that can prosecute “missing-self” cancers without antigen presentation. This is how you melt pancreatic tumors where PD-1 has nothing to grab.
· Re-sensitization mode: In CPI-refractory settings, MDNA11 renews TCF1⁺ progenitor CD8 T cells in the lymph nodes, restores chemokine traffic, and makes PD-1 antibodies relevant again. This is how you achieve partial responses in MSS colorectal cancer and endometrial subsets where PD-1 had failed.
Until recently, these were anchored to anecdotes: the PDAC complete remission (bypass) and the CRC partial response (re-sensitization). Both were compelling, but they risked feeling like one-off events.
That changed when two Nature Immunology papers from the Doherty Institute hit this summer, splashed in the press as a “breakthrough” ScienceX summary. Their conclusion: stem-like CD8 T cells don’t live in the tumor but in the lymph nodes, and checkpoints only succeed when those lymph nodes remain intact. Ablate the nodes, and response collapses.
The irony is that while Nature called this a new preclinical insight, Medicenna had already shown it clinically months earlier. At AACR 2025, MDNA11’s data demonstrated expansion of TCF1⁺ progenitor CD8s at the 90 µg/kg dose, with the strongest expansions in responders. And PRISM-11 had been public on this point just as the Doherty studies were landing:
Faces of EC (July 28, 2025): argued that even immune deserts could be converted if the lymph-node → progenitor → chemokine loop was preserved.
Faces of CRC (July 30, 2025): showed MDNA11 re-sensitizing PD-1 by re-seeding CD8 effectors from the lymph node niche.
The New Way (September 8, 2025): laid out the “Week-2/4 gate” framework in full, stitching cfDNA, chemokines, and TLS data into a single monitoring arc.
In other words, what Doherty has just proven in mice, Medicenna has already proven in people — and PRISM-11 was articulating the clinical version as or before the preclinical papers went live.
A Third Phenotype: Amplified Re-sensitization
The newly staged decks and Consensus data force us to add precision. In MSI-H, TMB-H, and virally driven tumors, MDNA11 doesn’t just re-sensitize — it supercharges the effect. The antigens are already abundant; what’s missing is renewal and traffic. Provide both, and the response is amplified: higher ORR, deeper CRs, steeper cfDNA drops.
MSI-H tumors: 50% ORR in mono patients.
Anal SCC: Complete remission in combination.
PDAC CRs labeled MSI-H in AACR/August decks: Previously treated as bypass archetypes, now better understood as amplified re-sensitization cases.
This third phenotype isn’t a new mechanism; it is a high-antigen variant of re-sensitization. The same progenitor renewal and chemokine surge occur, but on a richer substrate.
The Week-2/4 Truth Serum
In The New Way, we built the monitoring arc out of stovepiped evidence: cfDNA clearance in bladder cancer, chemokine correlations in melanoma, TLS density in ovarian and EC. It was bold synthesis, but it was also predictive.
The latest research now validates the arc as survival-linked and regulator-anchored:
Direct survival association:
– Caris ASCO 2025: TNBC patients on pembrolizumab with high CXCL9/10/CXCR3 signatures lived longer.
– Tokunaga (ER- breast) and Bronger (ovarian): CXCL9 expression tied directly to OS.Mechanistic clarity: Helmink et al. confirm TAMs as the dominant CXCL9 source in ICI patients.
Negative predictor: PNAS 2025 showed that patients with low CXCL9/10 had reduced PD-1 response — proving flat chemokine curves are predictive of failure.
Regulatory reinforcement: FDA’s 2023–24 guidance explicitly names cfDNA, chemokines, and TLS as “reasonably likely to predict benefit.”
Together, this makes the Week-2/4 gate more than monitoring. It is a protocol rule: if chemokines rise and cfDNA falls, stay the course. If they do not, escalate per pre-declared plan.
And the economics matter: replacing imaging-heavy monitoring with q2w liquid biopsy lowers per-patient trial monitoring costs by 40–60% while saving 6–10 months per trial.
A Map of Responders
To make this concrete, here’s how the latest MDNA11 responders fit into the three validated phenotypes — and what their bloodwork should look like at Week 2 and Week 4.
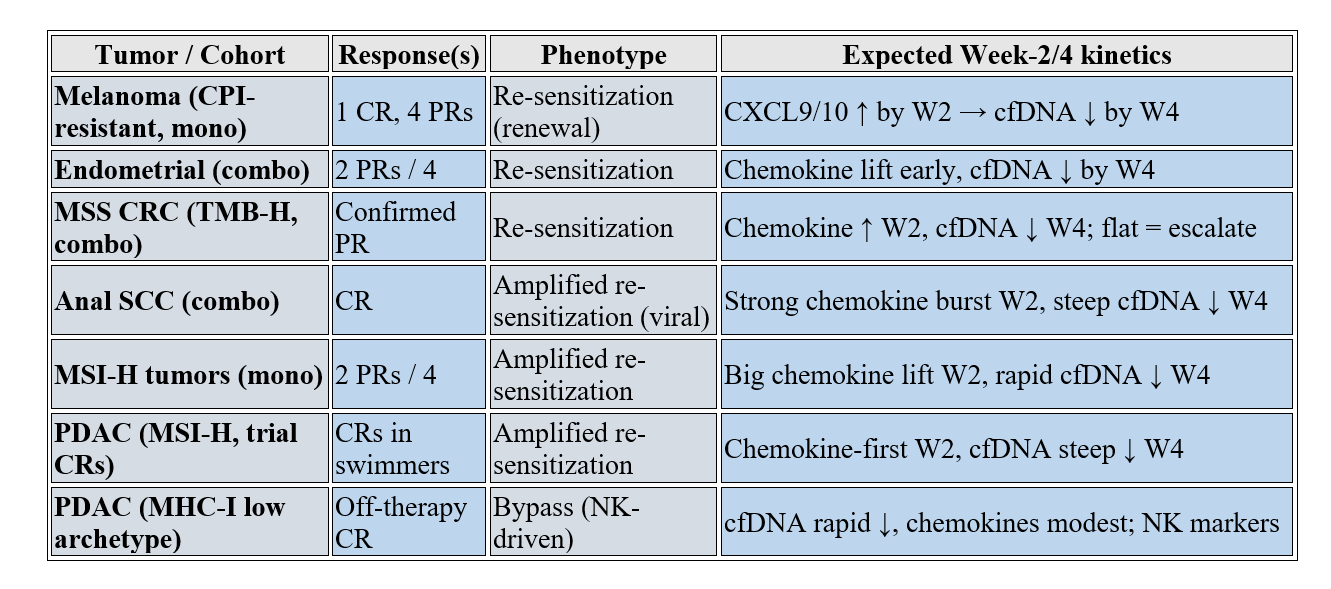
This table doesn’t create new buckets for their own sake. It clarifies that MDNA11’s biology plays out in predictable, monitorable paths — and that you can tell which one is in play by Week 2–4.
The Third Mode: STING and Timing
My original draft included the “third mode”: STING agonists paired with IL-2 to prosecute MHC-I–deficient tumors. That remains true, but the new research nuances it.
Consensus reviews confirm that STING agonism boosts antigen-presentation machinery and synergizes with IL-2, but also carries risk: given too early, it can damage lymph nodes and TLS formation. The right model is MDNA11 first, STING after. Prime the scaffold, then spark the innate loop.
That makes STING not a third independent bucket, but a sequencing partner whose timing determines whether it builds or burns.
Why Sequencing Matters More Than Ever
This isn’t just a detail about one drug pairing. It cuts to the heart of how MDNA11 should be used:
Front-of-line infrastructure protection: In indications where the current standard of care is destructive — radiation or chemotherapy that wipe out lymph nodes, TLS, or stromal scaffolds — MDNA11 belongs first. If you destroy the architecture before priming it, no downstream drug, checkpoint, or vaccine can work as intended.
Drug-level choreography: Even with targeted combinations, sequencing is the difference between synergy and sabotage. With STING, the order determines whether TLS are enhanced or burned out. With checkpoint inhibitors, MDNA11 should precede PD-1 or CTLA-4 to renew the progenitor pool and provide fresh effector targets. With triplet designs (e.g., ferroptotic locks, PARP/WNT inhibitors, or even ligase E3 constructs), MDNA11 again must come first, providing the lymph-node priming that allows subsequent layers to bite.
Tying Back to Old and New Frames
In earlier PRISM-11 frames (Rechallenge vs. Reprogramming), sequencing showed up implicitly — triplets for ferroptotic lock, salvage after CPI failure, layering reprogramming on top of rechallenge. What the new three-bucket frame adds is the real-time telemetry to know whether sequencing is working:
By Week 2 chemokines, you can see if the priming is happening.
By Week 4 cfDNA, you can know whether to add the next partner.
That transforms sequencing from a conceptual preference into an operational rule set.
Sidebar: The Platform of Sequencing
If MDNA11 is the scaffold, sequencing is the playbook. Every partner — checkpoint, STING, PARP, WNT, adenosine/TIGIT blockers, even ligase-based constructs — plugs into the same choreography:
Step 1: Prime the lymph node.
Step 2: Expand and renew TCF1⁺ progenitors.
Step 3: Trigger traffic (CXCL9/10/13).
Step 4: Layer checkpoint or innate agonists at the moment the system is most receptive.
Done in order, the system compounds. Done in reverse, it collapses.
The Big Picture
Sequencing is not a side note. It is the strategic hinge:
At the patient level, it dictates whether responses are durable or burn out.
At the trial level, it dictates whether signals appear strong enough for accelerated approval.
At the acquirer level, it dictates whether MDNA11 is seen as a single asset or the keystone of a combinatorial immunotherapy platform.
In short: MDNA11 first is not just a mechanistic argument. It is the only way sequencing works.
Proving the Point
All of this tightens the commercial and regulatory case.
Accelerated approval: With Week-2 chemokines and Week-4 cfDNA now survival-linked and FDA-recognized, Medicenna can pre-specify surrogate gates, cutting trial timelines by 6–10 months.
Commercial wedge: Amplified re-sensitization in MSI-H, TMB-H, and viral tumors creates near-term registrational cohorts with higher ORR and CR depth.
Competitive moat: No other IL-2 has shown activity across bypass, re-sensitization, and amplified re-sensitization, with monitoring that tells you which is in play by Week 4.
The burden of proof has shifted. What began as a bold synthesis in The New Way now stands as a validated, regulator-aligned framework. The anecdotes are no longer isolated; they are archetypes with kinetics, biomarkers, and trial rules attached.
That is how you prove the point.
References
Medicenna data (AACR 2025, Aug corporate deck, Sept HCW deck):
Durable monotherapy responses in CPI-resistant melanoma (1 CR, 4 PRs).
50% ORR in MSI-H mono subset; MSI-H labels in PDAC swimmer plots.
Anal SCC complete remission, EC partial responses in combo cohorts.
Expansion of TCF1⁺ CD8s at 90 µg/kg RDE; clean safety up to 120 µg/kg.
Bypass validation:
Ardolino M. et al., J Exp Med 2014: IL-2 rescues NK “missing-self” responsiveness.
Wolf Y. et al., PNAS 2022: IL-2 superkine + STING agonist cures MHC-I–deficient tumors via NK cells.
Gasteiger G. et al., Nat Immunol 2013: NK tuning in MHC-I–deficient contexts.
Re-sensitization validation:
Caris Life Sciences, ASCO 2025: High CXCL9/10/CXCR3 expression → survival in TNBC on pembrolizumab.
Tokunaga R. et al., Clin Cancer Res 2020: CXCL9 tied to OS in ER- breast cancer.
Bronger H. et al., Br J Cancer 2016: CXCL9 in ovarian cancer → improved OS.
House I. et al., PNAS 2025: Low CXCL9/10 expression predicts reduced PD-1 response.
Helmink B. et al., Nat Med 2020: TAMs as primary CXCL9 source post-ICI.
TLS / surrogate monitoring:
Dieu-Nosjean M.C. et al., Cancer Immunol Res 2022: CXCL13/TLS density predictive of ICI benefit.
Poschke I. et al., Nat Commun 2023: TLS density as survival-linked biomarker across tumors.
Li Y. et al., Front Immunol 2024: TLS/chemokines as predictive biomarkers.
Regulatory context:
FDA Draft Guidance (2023–24): cfDNA, chemokines, TLS density as “reasonably likely to predict benefit.”
Canon cross-references:
Droppings: PDAC Edition — bypass archetype.
Faces of CRC — re-sensitization archetype.
Faces of EC — progenitor + NK tandem in deserts.
The New Way — Week-2/4 monitoring arc (cfDNA + chemokine + TLS).
Consensus Research References
Mechanistic & Translational Gaps
NK cell IL-2 superkine tumor clearance
https://consensus.app/search/nk-cell-il2-superkine-tumor-clearance/nJy97OVFRiWqtVUD4g3ugw/
Surrogate & Monitoring Proof
CXCL9/10 immunotherapy survival linkage
https://consensus.app/search/cxcl9-cxcl10-immunotherapy-survival/Kp4msGW8R4uEr5Gz6WgDCg/
Comparative / Competitive Differentiation
Conditional masked IL-2 and lymph node priming
https://consensus.app/search/conditional-masked-il2-lymph-node-priming/ANHJBDNaThusxoLlrtfpEA/
Thanks again for the work you have put into this. Commentary from the “Scientists” out there is almost always of a negative and oppositional view, the fact that there is none speaks volumes.
Keep cookin’!
Hi David,
Have you managed to place any of your concepts in front of Medicenna's management? Are they aware of this?
I've held shares since 2018. I'm growing increasingly concerned with the inability to even get a partnership going let alone attract institutional interest. (I realize it OTC)
They are under one year from having to dilute current shareholders. From your research, things will become very expensive, very soon.
Regards
CC